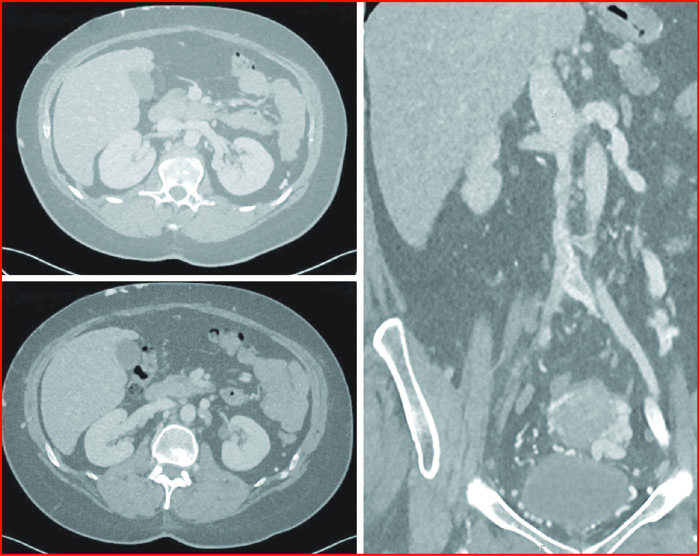
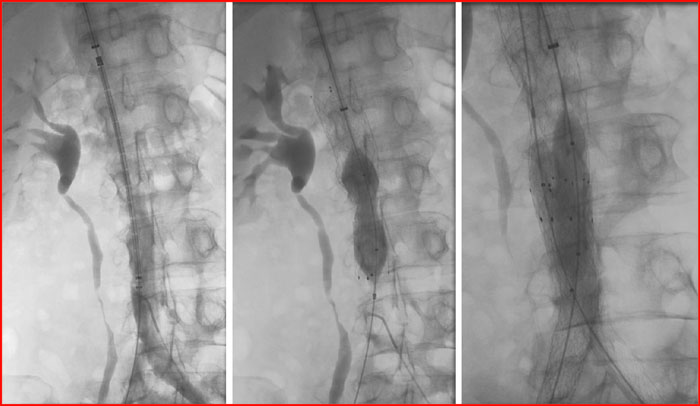
Coupes axiales et frontales au phléboscanner direct authentifiant l’occlusion de la veine fémorale commune et externe droite, la sténose serrée de la veine iliaque primitive gauche, la sténose diffuse de la veine cave inférieure (VCI) avec perméabilité des deux veines rénales.
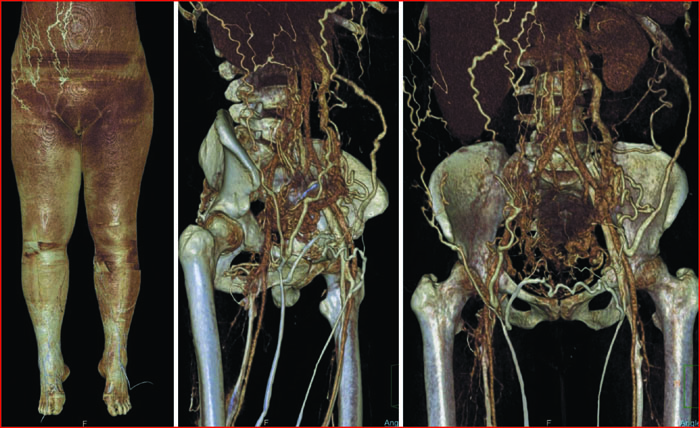
Reconstructions scanner en mode VRT (Volume Rendering) : augmentation de circonférence de la cuisse droite dans le cadre du syndrome post-thrombotique, riche dérivation collatérale (sous-cutanée, ovarienne, etc.) secondaire aux obstructions bi-iliaques et de la veine cave inférieure (VCI).
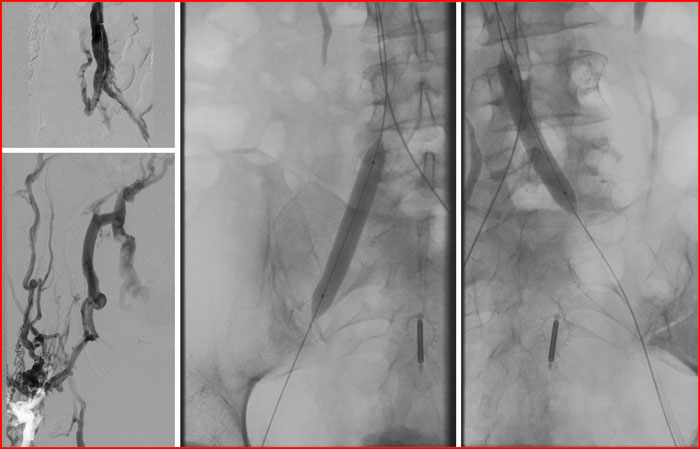
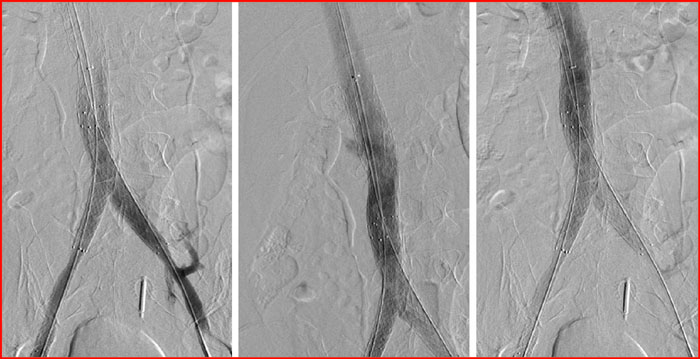
Mise en place d’un stent de 24 mm de diamètre dans la veine cave inférieure (VCI) et de stents de 12 mm dans les veines iliaques et fémorale commune droite.
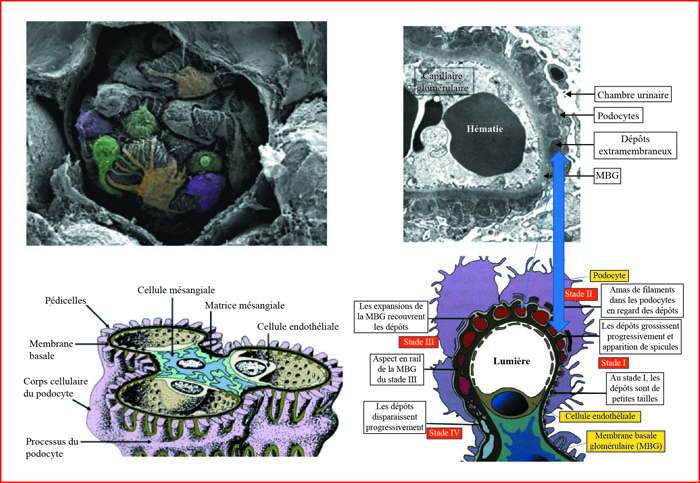
Aspect en microscopie électronique visualisant les dépôts denses aux électrons (correspondant aux dépôts d’immunoglobine G [IgG]) dans la partie externe de la membrane basale glomérulaire (MBG), sous les pieds des podocytes.
Les podocytes ou cellules viscérales épithéliales sont de volumineuses cellules en forme de pieuvre possédant une structure tridimentionnelle unique dans l’organisme.
Les podocytes ont un corps cellulaire globuleux contenant le noyau, des prolongements cellulaires primaires ou processus elicate, et des pédicelles qui reposent sur la membrane basale.
Les pédicelles sont des petites languettes cytoplasmiques qui reposent sur la basale capillaire, et qui ménagent, avec les pédicelles d’un podocyte adjacent, une sinueuse et elicate fente de filtration.
Il est d’usage de classer les glomérulonéphrites extramembraneuses (GEM) en quatre stades. Ces stades représentent les étapes successives d’un processus dynamique.
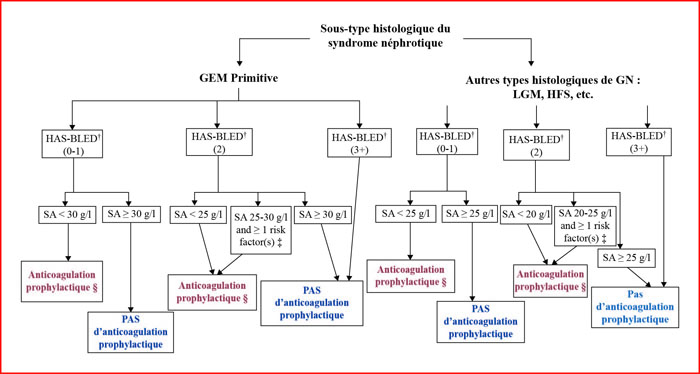
Algorithme pour l’approche suggérée de la prophylaxie de la thromboembolie chez les patients atteints de syndrome néphrotique (selon [77]).
† : scores HAS-BLED pour le risque de saignement. 0-1 : risque faible ; 2 : risque modéré ; 3-5 : risque élevé ; 5 : risque très élevé (voir tableau 2).
‡ : facteurs de risque supplémentaires. Protéinurie > 10 g/j, indice de masse corporelle > 35 kg/m2, prédisposition génétique documentée à la thromboembolie veineuse (TEV), immobilisation prolongée, chirurgie abdominale ou orthopédique récente, insuffisance cardiaque congestive de classe III à IV de la New York Heart Association.
§ : traitement de première intention de l’anticoagulation prophylactique : warfarine (rapport international normalisé [INR], 2,0-3,0) ou énoxaparine 40 mg/j.
Underlying causes of nephrotic syndrome (NS) include primary and secondary glomerulonephritis where membranous nephropathy (MN) is the most common cause in non-diabetic Caucasian adults over 40 years of age. Although it was recognised as a distinct clinicalpathological entity in 1940 by immunofluorescence and electron microscopy, the pathogenesis and treatment have become more apparent only in the last decade. Discovery of M-type phospholipase A2 receptor (PLA2R) antibodies has given new perspectives in understanding the pathogenesis of the disease process. Increased thromboembolic risk is a well recognized complication of nephrotic syndrome and MN, with variable reported incidence of deep venous thrombosis based on data in case series that mostly were reported more than a decade ago. The pathophysiology of hypercoagulability in the nephrotic syndrome is due to an imbalance of prothrombotic and antithrombotic factors, as well as impaired thrombolytic activities. Despite the well-established risk of venous thromboembolism (VTE) in nephrotic syndrome, the most effective method of VTE prophylaxis is unclear. We discuss the key questions to prophylactically anticoagulate adults with nephrotic syndrome.