Hépato-Gastro & Oncologie Digestive
MENUDuodenal neuroendocrine tumors Volume 26, issue 3, Mars 2019

- Key words: neuroendocrine tumor, duodenum, endoscopy, Vater ampula
- DOI : 10.1684/hpg.2019.1759
- Page(s) : 294-301
- Published in: 2019
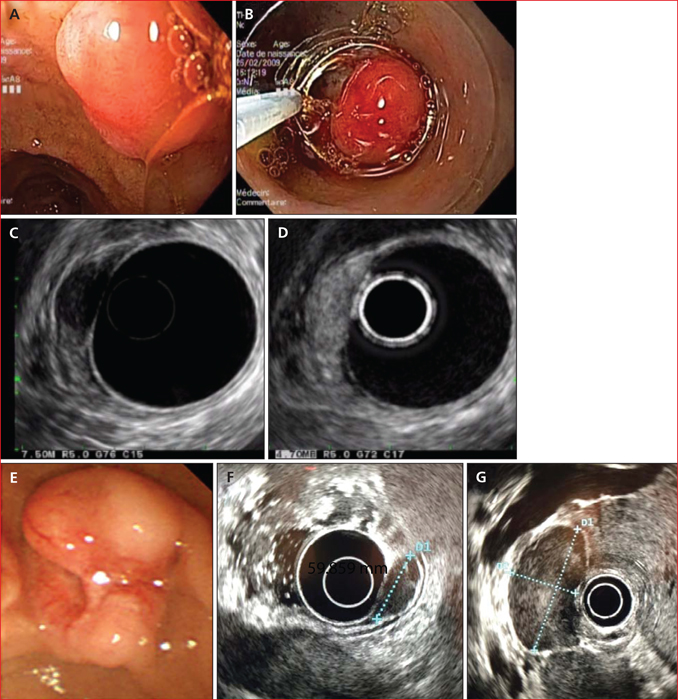
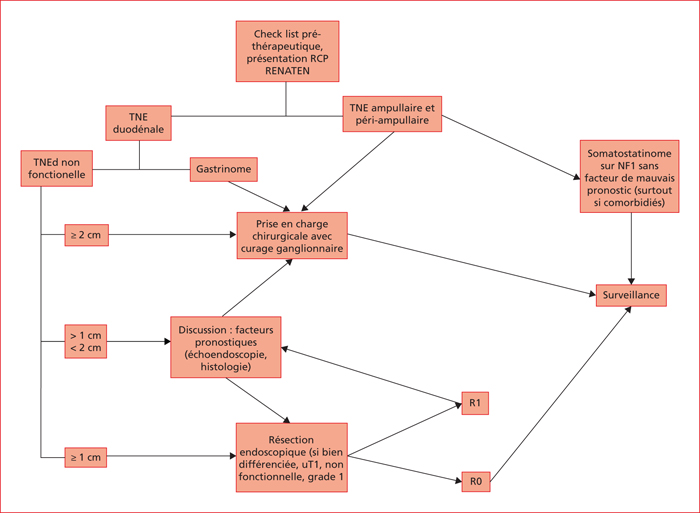
With the increasing frequency of upper gastrointestinal endoscopy examinations, endoscopists increasingly discover duodenal neuroendocrine tumours (dNET). dNETs represent only 1.9% of all neuroendocrine digestive neoplasms, but up to 3% of duodenal tumors. Approximately 81% of dNETs are localized at diagnosis. Lymph-node metastases and prognosis depend on the clinic, endoscopic and histopathologic features. The management of dNET should be validated in RENATEN tumor boards. dNETs under 1 cm in size, non-functioning and without poor prognostic factors should be removed endoscopically with the aim to achieve negative resection margins. Many endoscopic procedures exist, with variable effectiveness, and must be performed by trained operators. Radical surgery with lymphadenectomy is recommended for gastrinomas, dNETs >2 cm or in presence of lymph-node involvement at imaging or echoendoscopy. Treatment of lesions of intermediate size (1-2 cm) is not standardized and relies on prognostic criteria. For ampullary and periampullary NETs, size is not correlated with metastatic risk and lesions must be surgically removed. The recurrence profile is not well known and dNETs require long-term, local and systemic, follow up.
 This work is licensed under a
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
This work is licensed under a
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License