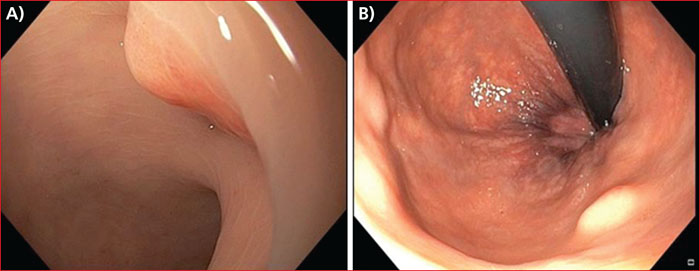
Présentation endoscopique d’une tumeur neuroendocrine du rectum en vision directe (A) et en rétrovision (B): nodule sous-muqueux jaune chamois (Photo du Docteur Vincent Lepilliez).
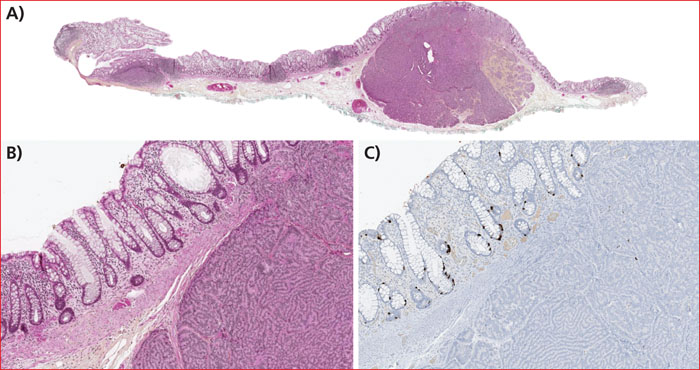
Aspect anatomopathologique d’une tumeur neuroendocrine du rectum (A, grossissement ×10 ; B, grossissement ×100 ; C, grossissement × 100, après immunomarquage à la chromogranine A, montrant l’absence de fixation des cellules tumorales habituelle dans cette localisation).
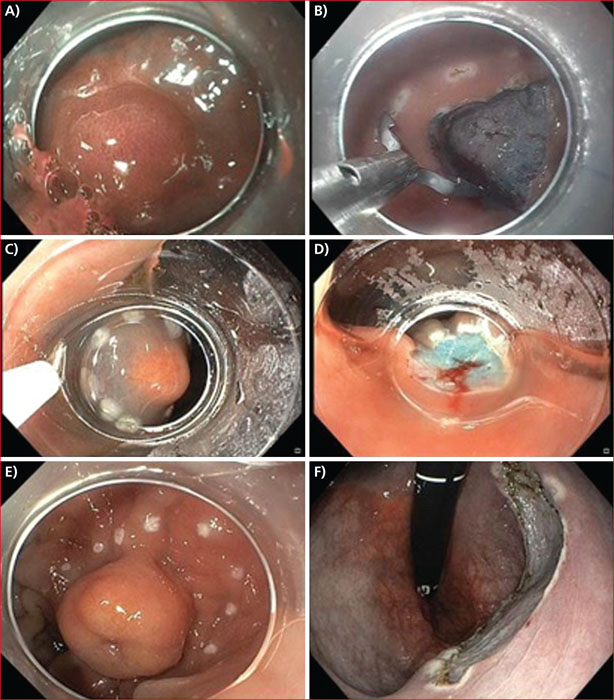
Images de résection endoscopique, par technique de mucosectomie au capuchon, avant resection (A), après marquage et soulèvement (C) et après résection (B et D) ; par technique de dissection sous-muqueuse, avant (E) et après (F) résection (Photos A et B du Dr Mathieu Pioche, Photos C, D, E, F du Dr Vincent Lepilliez).
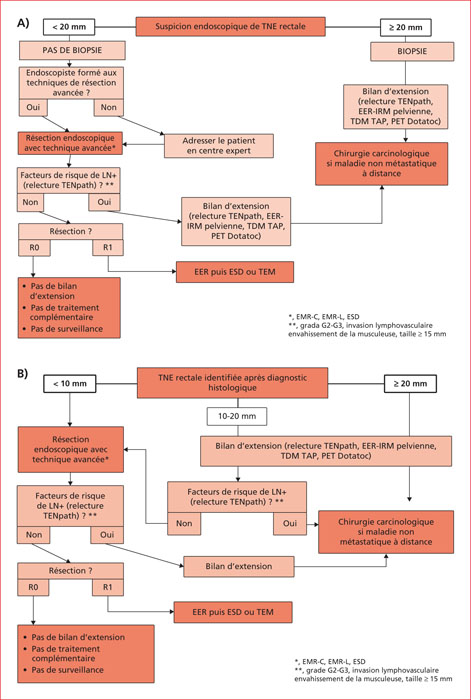
Algorithme de prise en charge d’une tumeur neuroendocrine rectale. A) Diagnostic fait endoscopiquement. B) Diagnostic obtenu après analyse anatomopathologique. EER-IRM : échoendoscopie rectale-imagerie par résonance magnétique. ESD : dissection sous-muqueuse endoscopique. PET Dotatoc : tomographie par émission de positons au Dotatoc. TDM TAP : tomodensitométrie thoraco-abdomino-pelvienne. TEM : exérèse trans-anale par microchirurgie endoscopique. TEP : tomographie par émission de positons.
The incidence of rectal neuroendocrine tumors (R-NET) increases, probably because of the colonoscopic colorectal cancer screening. R-NET represents about one third of all neuroendocrine tumors. They are localized at diagnostic in the majority of cases, metastatic forms count for 2 to 8% of tumors. The classic endoscopic aspect is a single yellow submucosal nodule. The metastatic prognostic mainly depends on the nodule size but also on histological factors as lymphovascular invasion, invasion of the muscularis, and a high histopronotic grade. R-NET less than 10 mm without poor prognostic factor should be removed endoscopically with negative resection margins and the patient does not require follow-up. At the opposite, R-NET larger than 20 mm needs scanographic extension assessment and carcinologic surgery. There is no consensual attitude for R-NET between 10 and 20 mm, an endoscopic resection is possible but a carcinologic surgery must be considered in the presence of poor prognostic factors.