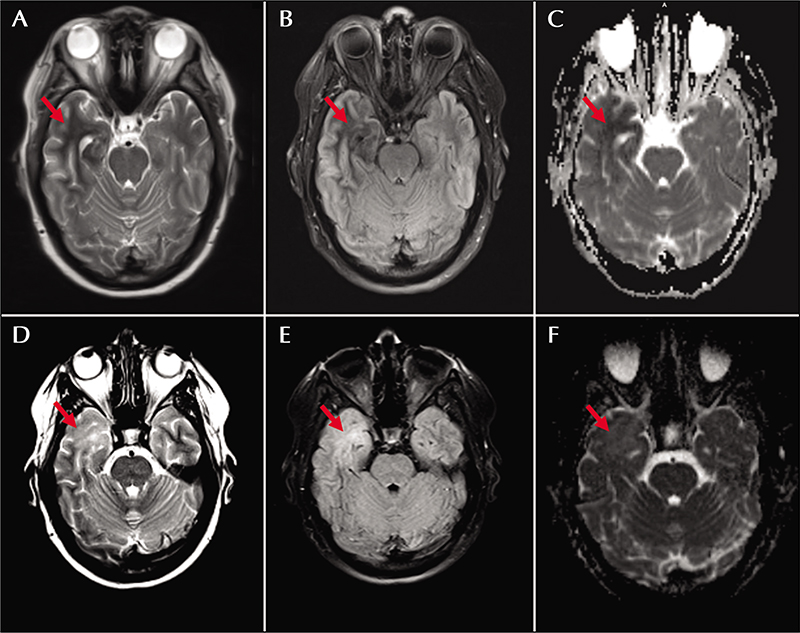
(A-F) A 47-year-old woman with headache and seizures in the setting of non-ketotic hyperglycemia. On initial presentation, T2-weighted (A) and FLAIR (B) images revealed a T2/FLAIR hypointense area within the right anterior temporal lobe associated with restricted diffusion on the ADC image (C). Two months following her initial presentation, there was interval development of T2 (D) / FLAIR (E) hyperintensity within the previously noted area of T2/FLAIR hypointensity in the anterior right temporal lobe with development of facilitated diffusion in this region, best visualized on the ADC image (F).
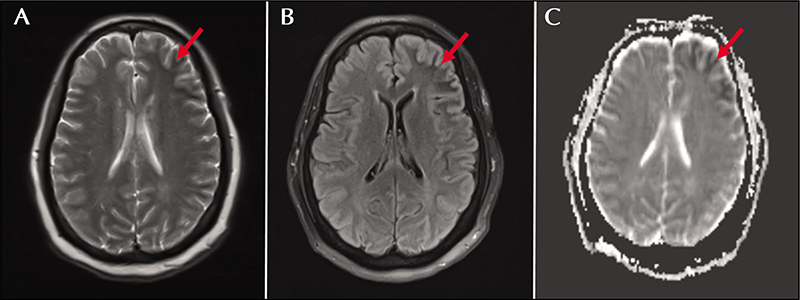
(A-C) A 57-year-old woman presented with altered mental status and seizures in the setting of non-ketotic hyperglycemia. T2 (A) and FLAIR (B) images demonstrate an area of T2/FLAIR hypointensity within the left frontotemporal lobes, which is associated with restricted diffusion, best visualized on the ADC image (C).
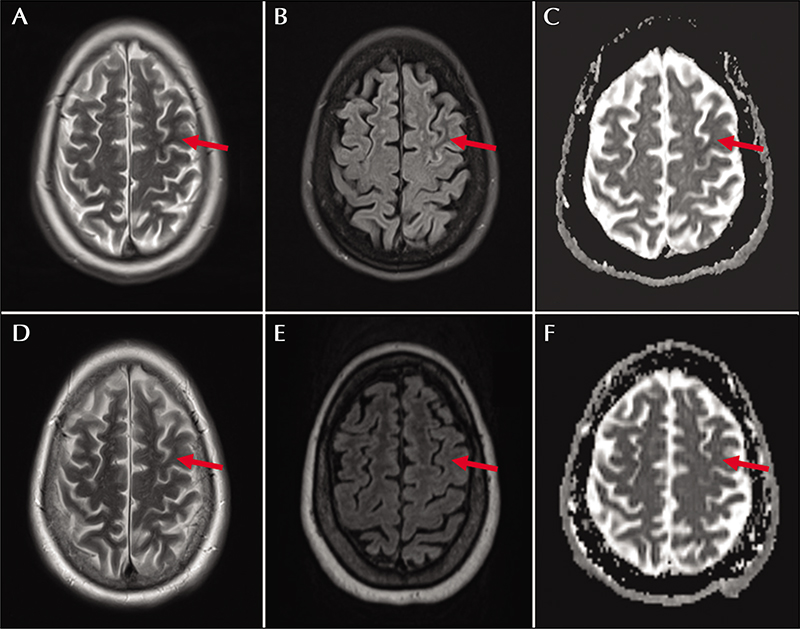
(A-C) A 60-year-old woman who presented with transient confusional spells was found to have seizures in the setting of non-ketotic hyperglycemia. T2 (A) and FLAIR (B) images showed an area of hypointensity in the left middle central gyrus, with mild diffusion restriction, best appreciated on the ADC image (C). Nine months following her initial presentation, there was interval resolution of these changes, as seen on the T2-weighted (D), FLAIR (E), and ADC (F) images.
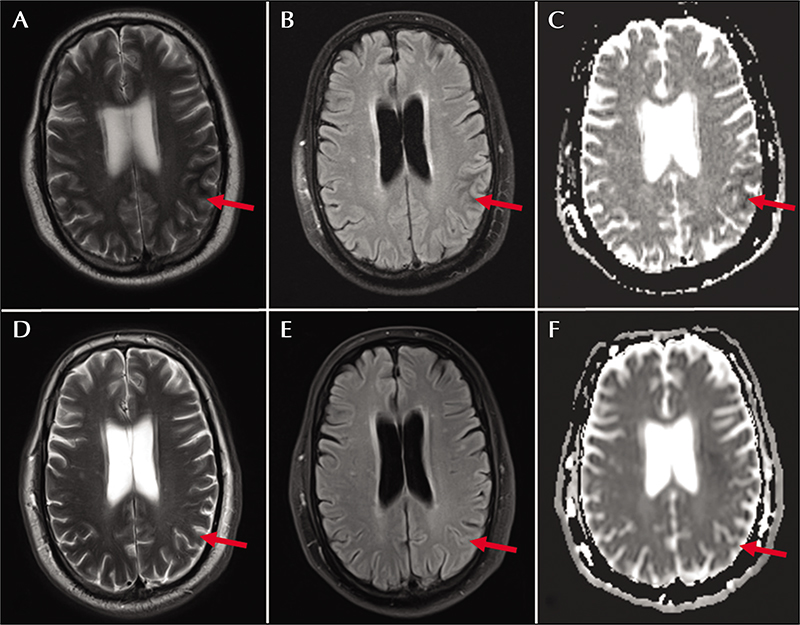
(A-F) A 56-year-old man with right hand jerks in the setting of non-ketotic hyperglycemia. On initial presentation, T2-weighted (A) and FLAIR (B) images revealed a T2/FLAIR hypointensity within the left parietal lobe with corresponding restricted diffusion (C) on the ADC image. Seven months after this presentation with correction of hyperglycemia, there was interval resolution of these changes, as seen on the T2-weighted (D), FLAIR (E), and ADC (F) images.
Non-ketotic hyperglycemia (NKH) is associated with a spectrum of symptoms and radiographic findings due to poorly-controlled diabetes mellitus. These lesions, which predominantly affect the parieto-occipital cortex, are commonly missed by neurologists and neuroradiologists due to their subtle hypointense appearance on T2-based imaging. We report four atypical cases of this syndrome to highlight its subtle, protean presentation in order to aid timely diagnosis. Based on our institutional case series, we describe four cases of NKH with atypical presentation and lesion burden affecting the anterior cortex. We review the clinical presentations, laboratory abnormalities, neuroimaging, and corresponding electroencephalography. Four patients with atypical NKH were characterized in our series. Presenting symptoms ranged from rhythmic handtapping to generalized tonic-clonic status epilepticus. Laboratory values were notable for marked hyperglycemia (range: 447 – 627 mg/dL), mild pseudohyponatremia (range: 127 – 136 mmol/L), and elevated hemoglobin A1C levels (range: 10.9 16.1%). All patients were found to have the classically described pattern of T2-based hypointensity; three with atypical distributions involving the “anterior” cortex. These lesions corresponded to the electrographic nidus of seizure burden. During follow-up, both seizures and T2-based hypointensity resolved within weeks of serum glucose normalization. Our series of four NKH patients with atypical findings of T2-based signal abnormalities expands the clinico-radiographic phenotype revealing a more protean distribution than previously described. Knowledge of these atypical imaging features will aid both the neurologist and radiologist in timely diagnosis and care of these patients.