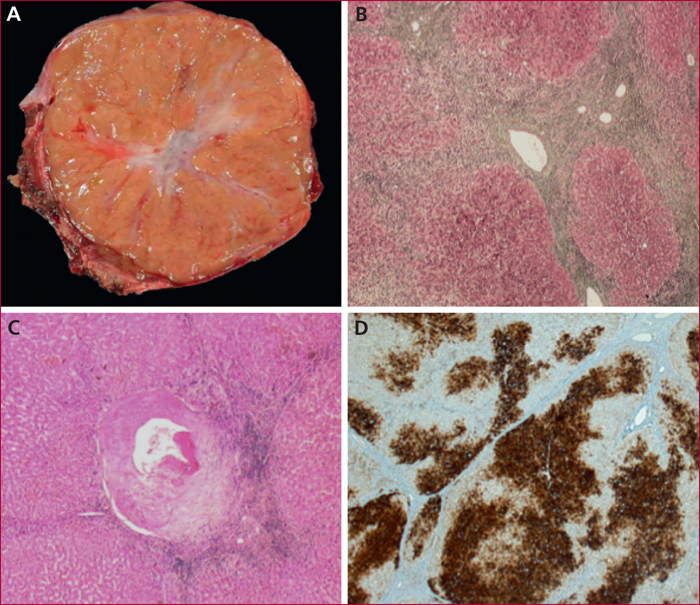
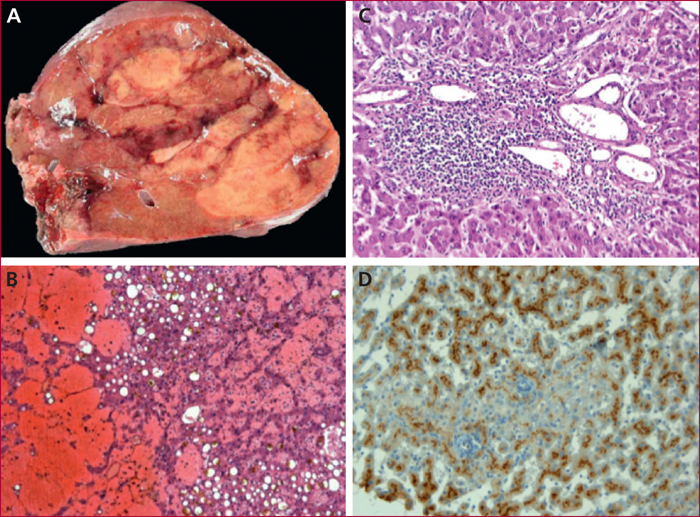
Hyperplasie nodulaire focale. A) Aspect macroscopique montrant un nodule bien limité, centré par une cicatrice fibreuse. B) Aspect microsopique mettant en évidence un nodule hépatocellulaire lobulé par des cloisons fibreuses (trichrome de Masson). C) Présence d’artères dystrophiques au sein des bandes fibreuses (hématéine-éosine-safran). D) Immunomarquage glutamine synthase : surexpression hépatocellulaire de la glutamine synthase réalisant un aspect en « carte de géographie ».
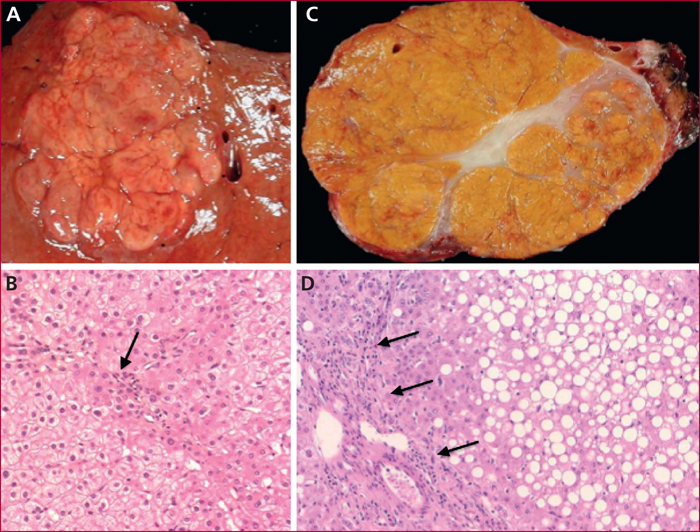
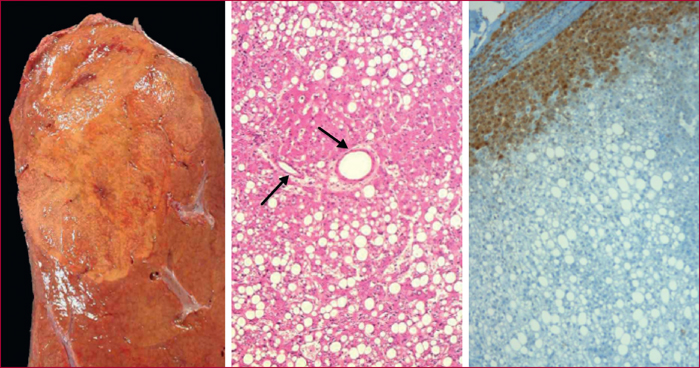
Absence de cicatrice fibreuse centrale : A) Aspect macroscopique montrant un nodule homogène lobulé mais sans cicatrice fibreuse centrale. B) Aspect histologique mettant en évidence une prolifération hépatocellulaire régulière, vaguement nodulaire, avec de rares ductules (flèches) (hématéine-éosine-safran). Stéatosique : C) Nodule bien limité centré par une cicatrice fibreuse de couleur jaune. D) La prolifération hépatocellulaire est préférentiellement stéatosique, bande fibreuse comportant des structures artérielles accompagnées par quelques éléments inflammatoires (flèches) (hématéine-éosine-safran).
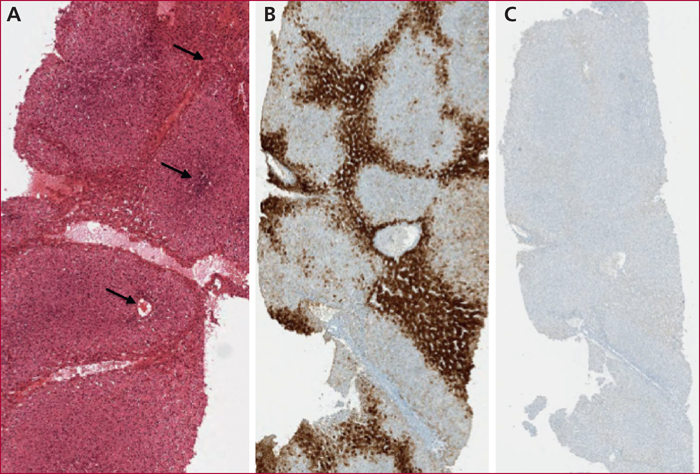
Hyperplasie nodulaire focale (biopsie). A) Aspect microscopique montrant une prolifération hépatocellulaire très bien différenciée montrant une architecture nodulaire avec quelques espaces fibrovasculaires sans septa (flèches) (hématéine-éosine-safran). B) Immunomarquage glutamine synthase : positivité hépatocellulaire avec aspect en « carte de géographie ». C) Immunomarquage sérum amyloïde A : absence d’expression de la prolifération hépatocellulaire.
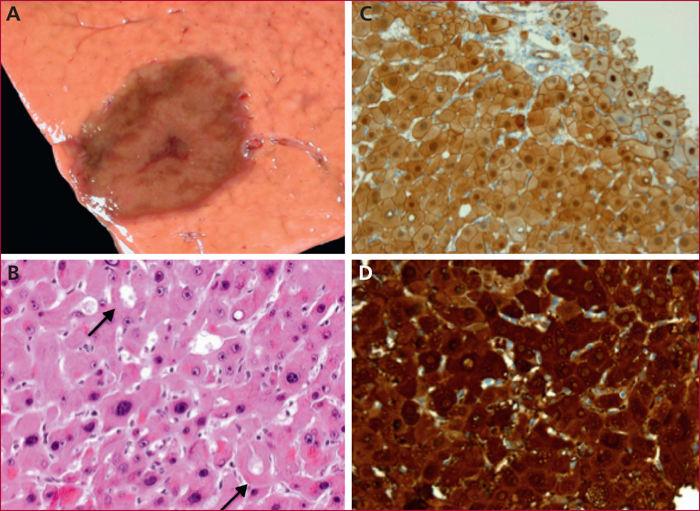
Adénome hépatocellulaire télangiectasique/inflammatoire. A) Aspect macroscopique montrant une lésion bien limitée, hétérogène, comportant des remaniements vasculaires en bandes. B) En histologie, la prolifération hépatocellulaire est très bien différenciée, trabéculaire, comportant des foyers de congestion sinusoïdale (télangiectasies). À noter, la présence d’hépatocytes stéatosiques (hématéine-éosine-safran). C) Présence d’artères peu épaisses regroupées en foyers, entourées de matrice extracellulaire inflammatoire (hématéine-éosine-safran). D) Immunomarquage sérum amyloïde A : positivité cytoplasmique de la plupart des hépatocytes tumoraux.
Adénome hépatocellulaire HNF1α muté. A) Aspect macroscopique montrant une lésion bien limitée, non encapsulée, jaune pâle, contrastant avec le foie non tumoral adjacent. B) En histologie, la prolifération hépatocellulaire est très bien différenciée, trabéculaire, majoritairement stéatosique. Quelques artères isolées à paroi fine sont notées (flèches) (hématéine-éosine-safran). C) Immunomarquage liver fatty acid binding protein : négativité de la prolifération tumorale contrastant avec la positivité hépatocytaire du foie non tumoral adjacent.
Adénome hépatocellulaire β-caténine activé. A) Aspect macroscopique montrant une lésion bien limitée, non encapsulée, de couleur brune développée au sein d’un parenchyme hépatique d’architecture normale. B) En histologie, la prolifération hépatocellulaire montre la présence d’atypies cytonucléaires et quelques structures pseudoglandulaires (flèches) (hématéine-éosine-safran). C) Immunomarquage β-caténine : positivité cytoplasmique et nucléaire des hépatocytes tumoraux. D) Immunomarquage glutamine synthase : positivité diffuse et intense de la prolifération tumorale.
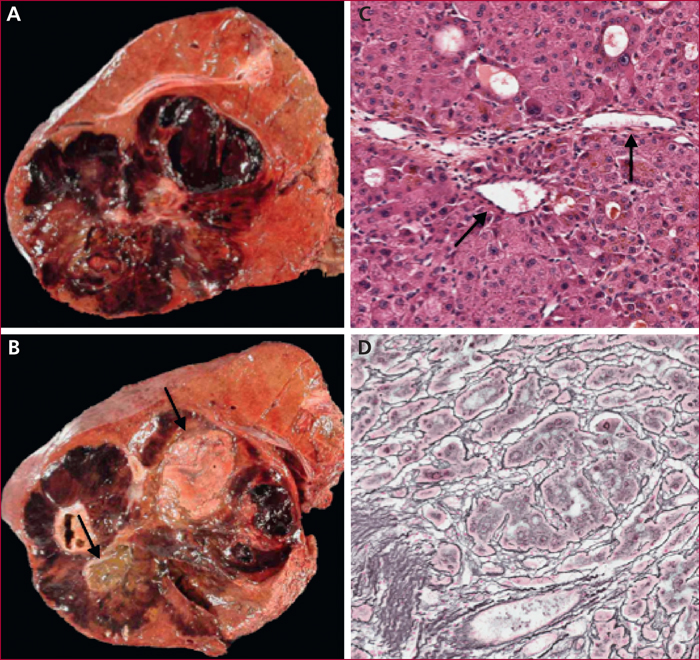
Adénomes hépatocellulaires (complications). A) Adénome hépatocellulaire hémorragique (aspect macroscopique) : le nodule tumoral est hétérogène avec plusieurs foyers hémorragiques. B) Adénome hépatocellulaire avec foyers de carcinome hépatocellulaire (aspect macroscopique) : lésion hétérogène comportant des foyers hémorragiques et des nodules charnus blanchâtres ou cholestatiques (flèches). C) En histologie, les foyers malins sont faits d’hépatocytes bien différenciés agencés en travées épaissies et en structures pseudo-glandulaires. Présence de quelques artères isolées (flèches) (hématéine-éosine-safran). D) Coloration de la réticuline montrant une fragmentation de la trame réticulinique soulignant des travées hépatocellulaires élargies carcinomateuses.
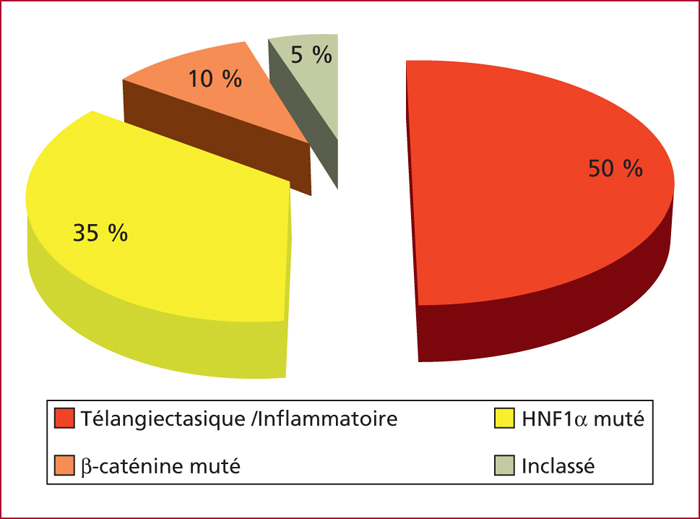
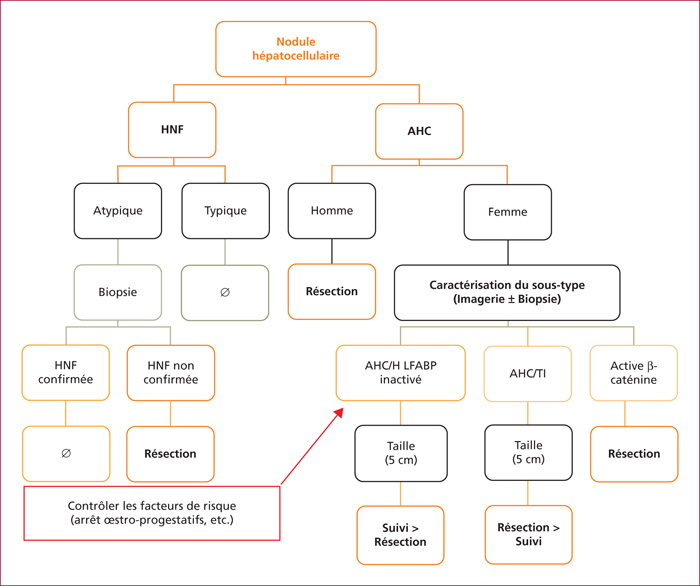
Benign hepatocellular tumors include 2 main entities, focal nodular hyperplasias (FNH) and hepatocellular adenomas (HCA). Both tumors, preferentially observed in young women without underlying chronic liver disease, display specific characteristics, in terms of pathophysiology, morphology and molecular features. Based on morphological and molecular characteristics, HCA are now recognized as a heterogeneous entity including 4 different subtypes (1) Telangiectatic/inflammatory, (2) Steatotic HNF1α inactivated, (3) β-catenin activated and (4) unclassifed. Importantly, pathomolecular classification has significant clinical impact outlining higher risk of complications, hemorrage in Telangiectatic/inflammatory subtype, and malignant transformation towards hepatocellular carcinoma in β-catenin activated. Regarding management, abstention remains the rule in the vast majority of FNH, while follow-up or surgical resection are recommended for HCA according to 3 criteria including gender, HCA subtype and size.