Jerking during absences: video-EEG and polygraphy of epileptic myoclonus associated with two paediatric epilepsy syndromes
Volume 23, issue 1, February 2021
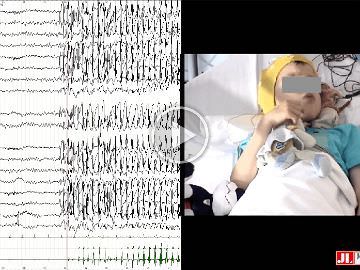
Ictal EEG (video sequence 1) with EMG on both deltoids (DELT D: right; DELT G: left) in Patient 1. Seizure starts with bilateral frontal-temporal spikes and polyspike and waves with a more marked amplitude on the right side, followed by rhythmic bilateral synchronous spike waves (SW) at 3 Hz with maximal amplitude over the right frontal-temporal areas, lasting around 20 seconds. Note bilateral rhythmic contractions predominating on the left deltoid (DELT G).
Ictal EEG with EMG on both deltoids (DELT D: right; DELT G: left) in Patient 1 with narrow window (A) illustrating the complex relationship between spikes and EMG contractions, and bilateral rhythmic deltoid contractions predominating on the left, increasing in duration and superposed on a gradual increase in muscular tone of both deltoids predominating on the left. Note an inhibitory component of the tonic activity between myoclonia interrupted by post-myoclonic silent periods. (B) Focus on spikes and their relationship awith EMG contractions.
Back-averaging locked to the onset of myoclonic jerks during the myoclonic absence in Patient 1 using two different subsets of the first myoclonic jerks, (A) (n=32) and (B) (n=44), revealing bilateral synchronous spikes with a positive component at frontal (Fz, F3, F4) electrodes and a negative component at temporal-occipital electrodes, predominating on the right and preceding the myoclonic jerk by 20-30 ms. (C) The pre-myoclonic spike is represented on a 2D map illustrating bilateral tangential dipoles with inversion of polarity near central electrodes, predominant on the right.
Ictal EEG (video sequence 2) with EMG of both deltoids and the neck (DELT D: right; DELT G: left; EMG3: neck) in Patient 2 showing a sequence of high-amplitude 2-3-Hz SW during up to 20 seconds with maximal amplitude over the right central-parietal area. Note bilateral rhythmic contractions predominating on the left deltoid corresponding to a sudden recovery of muscle tone after negative myoclonus on both deltoids.
Ictal EEG (video sequence 2) with EMG of both deltoids and the neck (DELT D: right; DELT G: left; EMG3: neck) in Patient 2 with (A) the narrow window showing the sequence of diffuse, high-amplitude, 2-3-Hz SW with maximal amplitude over the right central-parietal area. The positive transient of the spike-wave shape on the right preceded that of the left. Note the relationship between the SW and the muscular contractions corresponding to the sudden recovery of muscle tone of both deltoids after the negative myoclonus. (B) Ictal EEG (video sequence 3) with EMG of both deltoids and the neck (DELT D: right; DELT G: left; EMG3: neck) in Patient 2 showing short bursts of bilateral, high-amplitude 2-3-Hz SW with maximal amplitude over the right central-parietal area. On EMG, note the contractions of both deltoids during the sequences of the SW and isolated negative myoclonias of the left deltoid and trapezius following a right central SW. EMG of the left deltoid and he neck showed a negative myoclonus lasting between 150 ms and 270 ms.
(A, B) Back-averaging in two subsets of jerks, (A) (n=66) and (B) (n=44), locked to the onset of the sudden recovery of muscle tone of both deltoids in Patient 2, revealed a central right negative SW in which the spike preceded the contraction with a variable latency of 240-330 ms. (C) Back-averaging using six isolated jerks.
Back-averaging locked to the onset of negative myoclonus of the left deltoid in Patient 2 using three subsets of events, (A) (n=66), (B) (n=43), (C) (n=7), showing a right central SW preceding the onset of the negative myoclonus by 20-40 ms. (D) 2D mapping of the same SW showing a right central tangential dipole.
(A, B) Back-averaging, locked to the onset of the isolated negative myoclonus on the left deltoid in Patient 2 (video sequence 3) showing a right central SW with latency of 50-60 ms. (C) Back-averaging locked to the onset of sudden recovery of muscle tone of both deltoids following a right central SW with a latency of 240 ms. (D) 2D map locked on the right central spike of the SW from (C) showing right frontal-central tangential dipole.
EEG during slow-wave sleep in Patient 2. Note the bilateral synchronous continuous spike waves of 1-2 Hz, predominant on the right during the whole duration of NREM sleep, visible on the spectral density analysis at C4 and C3 over a period of nine hours (lower panel).
Epileptic myoclonus (EM) is reported in many paediatric epilepsies from neonatal period to adolescence. Myoclonus can be the only seizure type or may occur among others, independently or in combination as a single ictal event. We report two children presenting with absences associated with myoclonus, predominating on one side, in a setting of two different types of absence seizures and two different electro-clinical syndromes.
Methods
Patients were explored with long-duration video-EEG coupled to surface EMG polygraphy. EEG was visually analysed and complemented by jerk-locked back-averaging.
Results
Two types of seizure, encompassing myoclonus and absence, were identified: myoclonic absences in the context of epilepsy with myoclonic absences and atypical absences with atonic component (negative myoclonus) in the context of encephalopathy related to status epilepticus during slow sleep (ESES). In the latter case, rhythmic upper limb jerking, mimicking positive myoclonus, corresponded to recovery of muscular tone after each negative myoclonus.
Significance
Due to the rhythmic recovery of muscle tone, subsequent rhythmic negative myoclonus may exhibit a similar clinical picture to that of rhythmic positive myoclonus. Video-EEG recording coupled to EMG polygraphy is essential in order to precisely characterize motor manifestations during seizures with myoclonus [Published with video sequences].