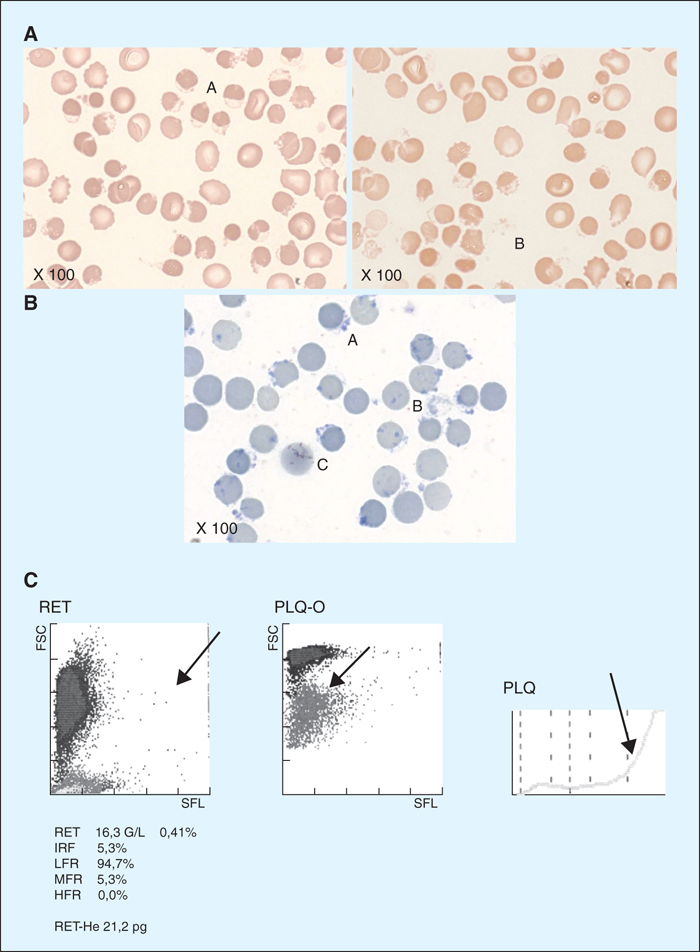
Aspect cytologique des hématies et données de la NFS sur l’automate XE 2100, Sysmex® - 3 jours après le début des symptômes. A. Frottis sanguin (X100) montrant la présence de nombreux hemighosts (A) et quelques ghosts (B). B. Frottis sanguin coloré au bleu de crésyl, montrant des corps de Heinz, notamment dans des hemighosts (A) et des ghosts (B). À noter la présence d’un réticulocyte (C). C. Graphes de l’automate XE 2100, Sysmex®. Diagramme RET : réticulocytes - volume (FSC) en ordonnée, fluorescence (SFL) en abscisse. La flèche souligne la pauvreté en fraction immature (IRF). Diagramme PLQ-O : plaquettes fluorescentes, mode optique de mesure. La flèche montre l’interférence des formes ghosts. Diagramme PLQ : plaquettes mesurées par impédance. La flèche montre l’interférence avec les hématies de petit volume.
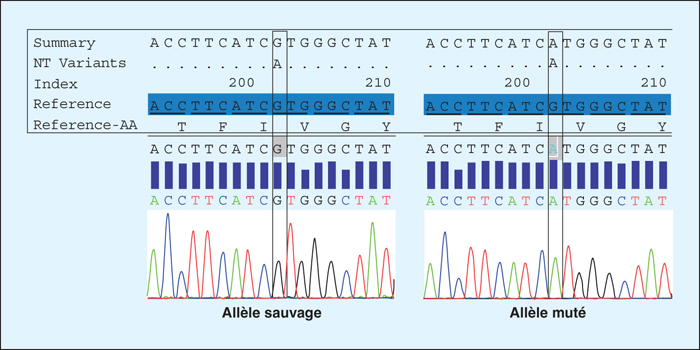
Description de la mutation hémizygote de l’exon 4 du gène de la G6PD, c.202G>A (p.Val68Met) associé au variant A-, le plus fréquemment rencontré dans les populations africaines, et responsable de la synthèse d’une enzyme instable. Il correspond à la classe III de l’OMS.
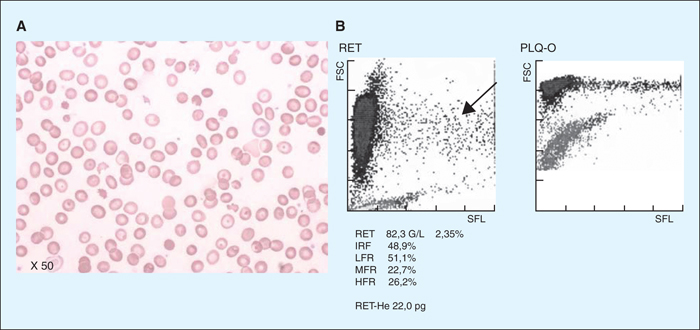
Aspect cytologique des hématies et données de la NFS sur l’automate XE 2100, Sysmex® - 7 jours après le début des symptômes. A. Frottis sanguin (X50). B. Graphes de l’automate XE 2100, Sysmex®. On observe la génération de jeunes réticulocytes (HFR, flèche sur le diagramme).
We report the case of a 2 year-old boy hospitalized into the emergency room for influenza pneumonia infection. The evolution was marked by a respiratory distress syndrome, a severe hemolytic anemia, associated with thrombocytopenia and kidney failure. First, a diagnosis of hemolytic uremic syndrome (HUS) has been judiciously suggested due to the classical triad: kidney failure, hemolytic anemia and thrombocytopenia. But, strikingly, blood smears do not exhibit schizocytes, but instead ghosts and hemighosts, some characteristic features of a glucose-6-phosphate dehydrogenase deficiency. Our hypothesis has been confirmed by enzymatic dosage and molecular biology. The unusual initial aplastic feature of this anemia could be the result of a transient erythroblastopenia due to the viral agent, at the origin of the G6PD crisis on a background of a major erythrocyte anti-oxydant enzyme defect. This case of G6PD defect points out the continuously importance of the cytology, which was able to redirect the diagnosis by the hemighost and ghost detection.