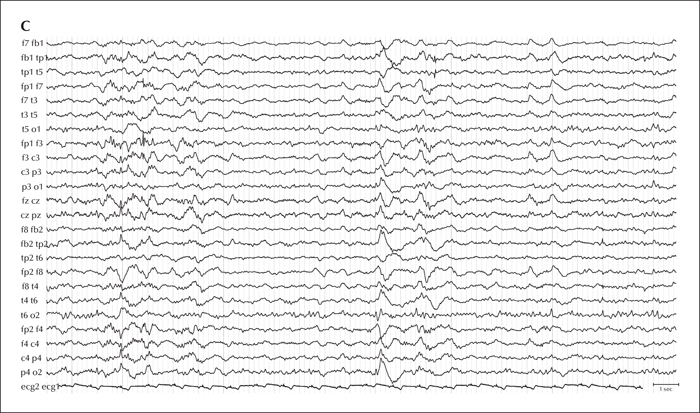
Distribution of interictal epileptiform discharges (IEDs) on scalp EEG. (A) The majority of IEDs were present in the left-sided fronto-temporal area (phase reversal at electrodes Fb1, T3). (B) There were also less frequent IEDs over the right-sided frontal area (phase reversal at electrodes F4). (C) Rarely, IEDs could be found over the left frontal regions (phase reversal at electrode F3).
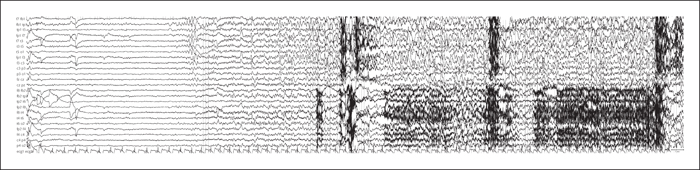
Ictal scalp EEG showing the typical pattern for the patient. The seizures started with a short flattening over the left anterior temporal lobe, followed by irregular theta waves in the same area. After, clear-cut rhythmic activity appeared; this rhythmic activity started on the left side, but rapidly spread over the right hemisphere. The left-sided ictal activity predominated throughout the entire seizure.
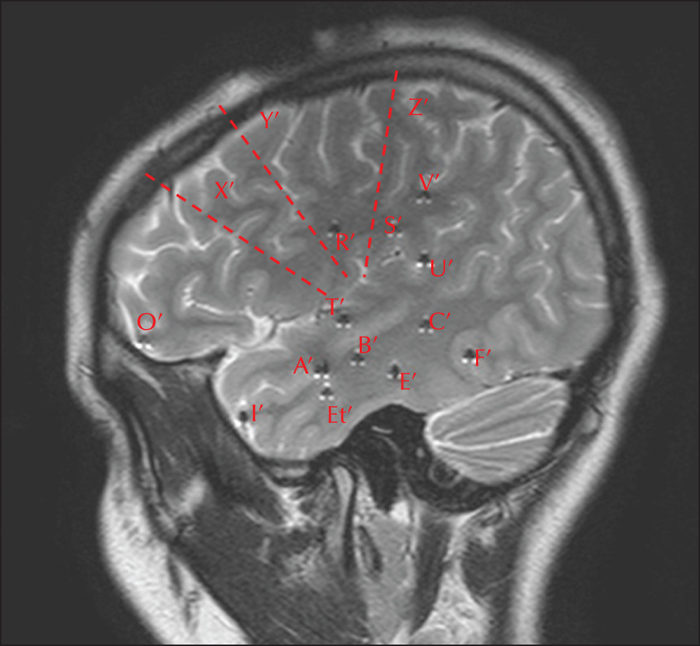
Electrode positions for invasive EEG monitoring. The positions of electrodes in the left temporal lobe are the following: A’: amygdala; B’: anterior hippocampus; C’: posterior hippocampus; I’: temporal pole; Et’: entorhinal cortex; T’, U’: temporal operculum; E’, F’: temporobasal region. The positions of electrodes in the left extra-temporal lobe structures are the following: O’: fronto-orbital cortex; R’: frontal operculum; S’: parietal operculum; V’: cingulum (posterior part); X’: anterior insula (dotted line); Y’: posterior insula (dotted line); Z’ (dotted line).
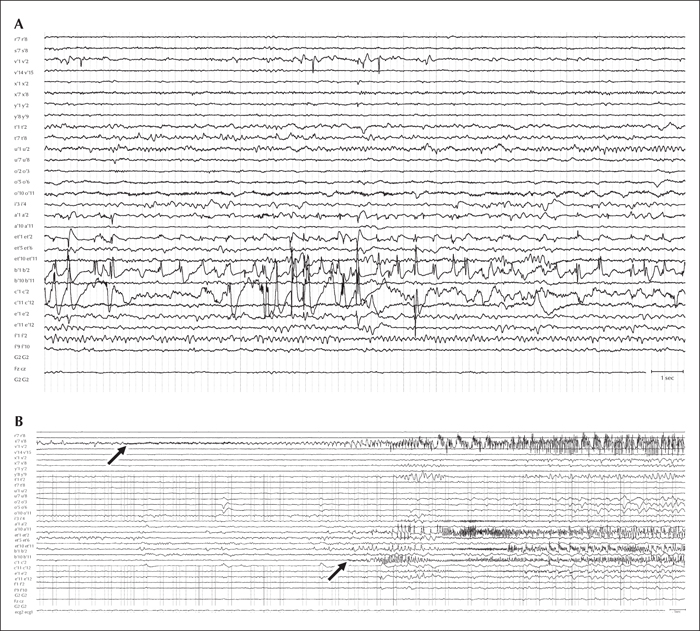
The results of invasive EEG. (A) Distribution of interictal epileptiform discharges (IEDs) on invasive EEG. IEDs dominated in the area of left-sided mesiotemporal structures (left amygdala: electrode Á1-2; left entorhinal cortex: electrode Et́1-2; and left hippocampus: electrodes B́1-2 and Ć1-2), but there were also IEDs and bursts of rapid activity (blue arrow) in the area of the left posterior cingulum (electrode V́1-2). (B) Ictal findings on invasive EEG. The seizures started with low-voltage fast (LVF) activity in the left side of the posterior cingulum (first arrow); LVF activity propagated to the left-sided mesiotemporal structures, where the symptomatogenic zone was localized (second arrow).
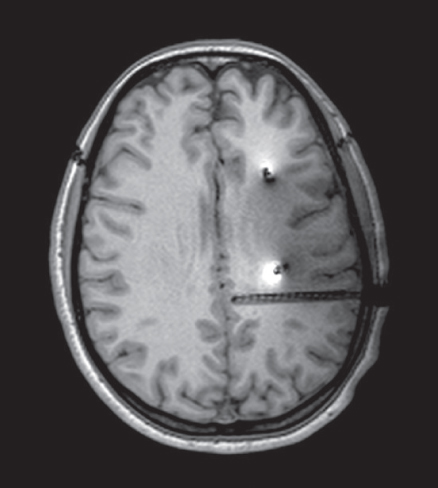
More detailed view of the position of electrode V́. The low-voltage fast activity started in the mesial contacts of this electrode, encompassing the left side of the posterior cingulum, as seen in this image.
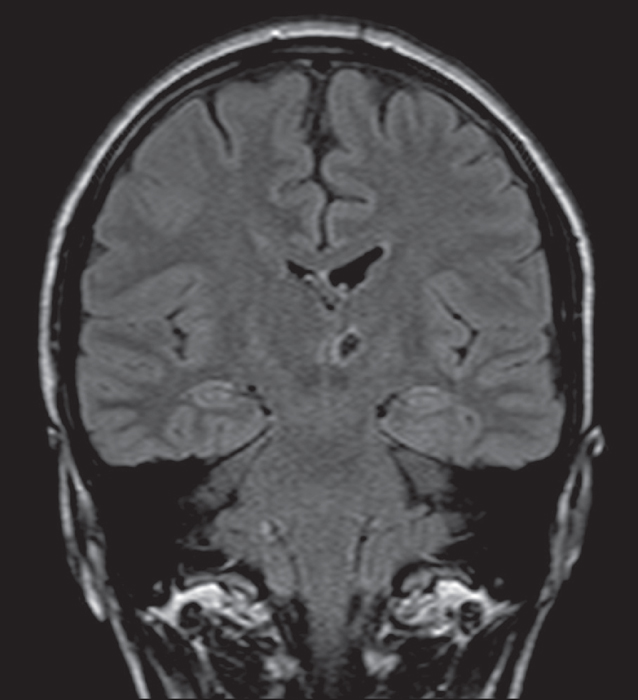
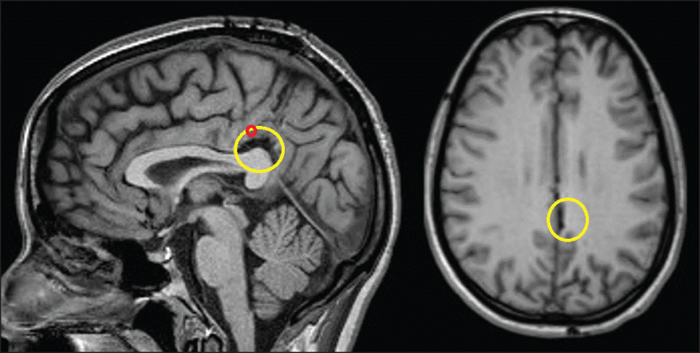
The second preoperative MRI. We retrospectively identified a discrete change on MRI (yellow circle). The position of seizure onsets is marked by red dots.
1 Brno Epilepsy Center, First Department of Neurology, St. Anne's University Hospital and Faculty of Medicine, Masaryk University
2 Central European Institute of Technology (CEITEC), Masaryk University, Brno, Czech Republic
3 Clinique de Neurologie, University Hospital of Grenoble, France
* Correspondence: Irena Doležalová
Brno Epilepsy Center,
First Department of Neurology,
St. Anne's University Hospital and Faculty of Medicine,
Masaryk University,
Pekarska 53, Brno 65691
Czech Republic
Temporal lobe epilepsy is the most frequent form of drug-resistant epilepsy referred to epilepsy surgery centres. The vast majority of lesional cases can be operated on without invasive investigation which is often not the case for non-lesional cases. Invasive investigation in non-lesional cases, however, may lead to unexpected results, as illustrated in the following case report. [Published with video sequence on www.epilepticdisorders.com]