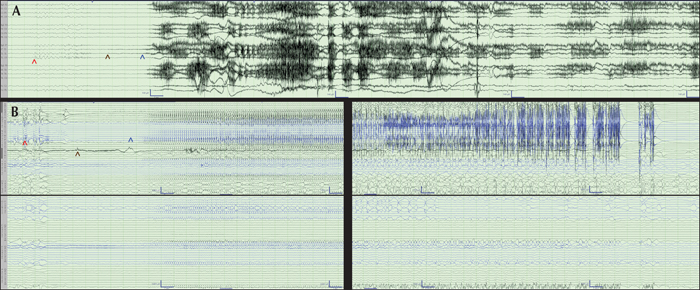
Scalp EEG and stereo-EEG recordings of a 41-year-old patient with mirthful laughter seizures. (A) Ictal scalp-EEG: a total of five stereotypical mirthful laughter seizures were recorded in which EEG changes preceded clinical changes. Seizures began over A1-T3-F7 with polyspikes and spread to C3-P3 over five seconds. This was followed by generalized low-voltage fast activity with maximum left temporal activity, followed by muscle artefacts when the patient started laughing. (B) Ictal stereo-EEG (bipolar montage): during two weeks of intracranial electroencephalographic monitoring, 23 seizures were recorded, all electrographically stereotyped and preceding the clinical onset by three to four seconds. Onset with 1.5 Hz and high-voltage discharges were located in the left neocortical temporal region, and -to a lesser degree- in the amygdala, insula, and orbitofrontal cortex (compare with figure 2B). This was followed by low-voltage fast activity in the same electrodes (maximum in the neocortical temporal regions) for two seconds. After that, there was a diffuse attenuation in all the contacts for five to six seconds. Finally, spikes progressively built up in the temporal neocortex, which then spread to the rest of the temporal region, as well as to the amygdala, insula, and orbitofrontal cortex. In order to downsize the figure, 51 seconds of the ictal stereo-EEG have been cropped. Red marker: electrographic onset; brown marker: awaking from sleep; blue arrow: clinical seizure onset (laughter); hc: hippocampus.
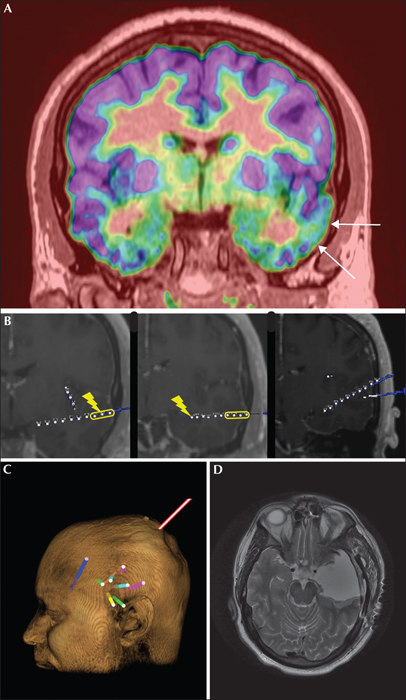
(A) Left temporal hypometabolism (arrows) in a patient with mirthful laughter seizures demonstrated by 18F-fludeoxyglucose positron emission tomography. (B) The left, middle, and right panel show the depth electrode contacts at the level of the amygdala, as well as the anterior and posterior hippocampus, respectively. The neocortical seizure onset zones are highlighted with yellow boxes. Stimulation of one contact in the anterior superior temporal gyrus neocortex electrode (left panel; lightening symbol) triggered a typical laughing seizure at 2 mA. Stimulation of the anterior hippocampus electrode contact (middle panel; lightning symbol) with 2 mA triggered epigastric rising, nausea, and induced speech arrest, and made the patient feel as if he was going to have a laughter seizure. (C) Stereoelectroencephalography implantation scheme covering the left temporal (lower row: yellow/green/pink electrodes) and orbitofrontal lobe (dark blue electrode), the opercular region (upper row: light green/light blue/pink electrodes), as well as the insula (light blue and oblique red electrode). (D) T2-weighted magnetic resonance imaging after left anterior temporal lobectomy.
We provide an overview of the surgical outcome of extra-hypothalamic epilepsies with gelastic seizures based on an original case report and a summary of the literature. Twenty-two articles providing information on the outcome of resective surgery in 39 patients with extra-hypothalamic gelastic seizures from the temporal (19 patients) or frontal lobe (20 patients) were selected. We add another case of temporal lobe gelastic seizures to the literature with a video demonstrating the mirthful component of this patient's laughing seizures. Drug-refractory cases of gelastic seizures from the temporal or frontal lobes are amenable to surgical treatment following thorough investigation with imaging, as well as scalp and intracranial EEG.