Epileptic Disorders
MENUEpilepsy in inborn errors of metabolism Volume 7, numéro 2, June 2005

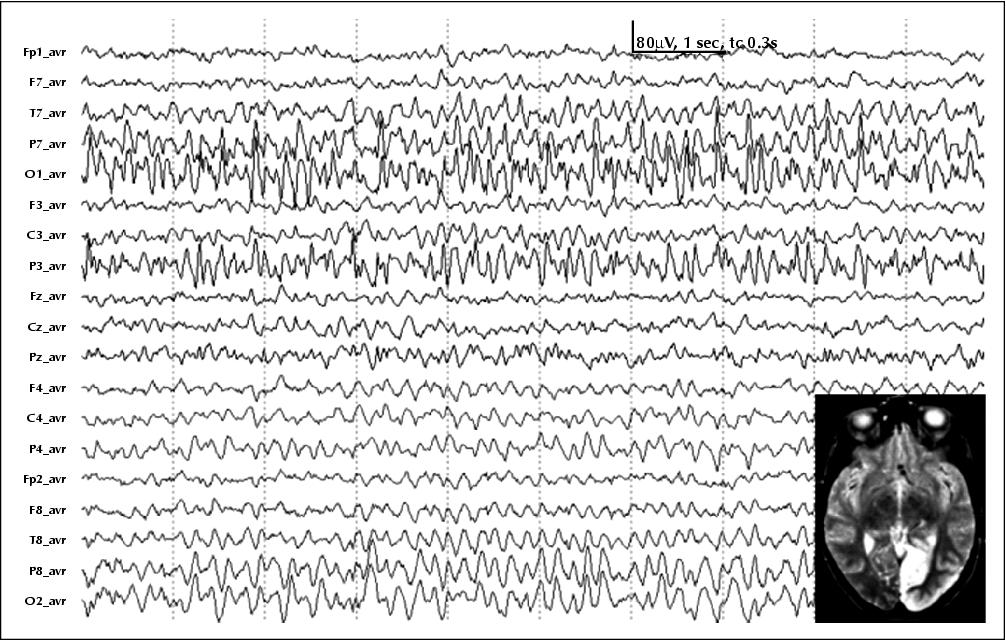
Figure 1 EEG (average reference) of a patient with MELAS syndrome in an acute, stroke-like episode demonstrating an ongoing seizure over the left parieto-occipital region corresponding to the involved brain area on T2w MRI.

Figure 2 EEG of a child with the GAMT defect under creatine supplementation (A) and creatine supplementation plus ornithine-rich arginine-reduced diet (B). The child was in a non-convulsive status epilepticus with a nearly continuous generalised spike-wave pattern before the diet was started (A). Under diet, non-convulsive status stopped (B).
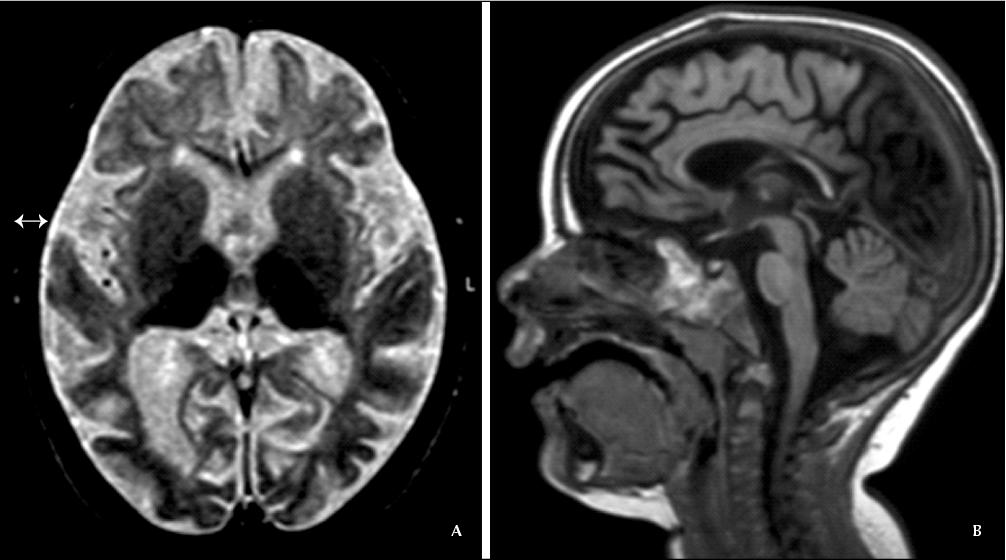
Figure 3 (A) Axial T2w image and (B) sagittal T1w image of a 12 month-old child with infantile neuronal ceroid lipofuscinosis. The supratentorial atrophy of both grey and white matter is severe, compared with a relatively intact cerebellum. Signal from both thalami is hypointense.
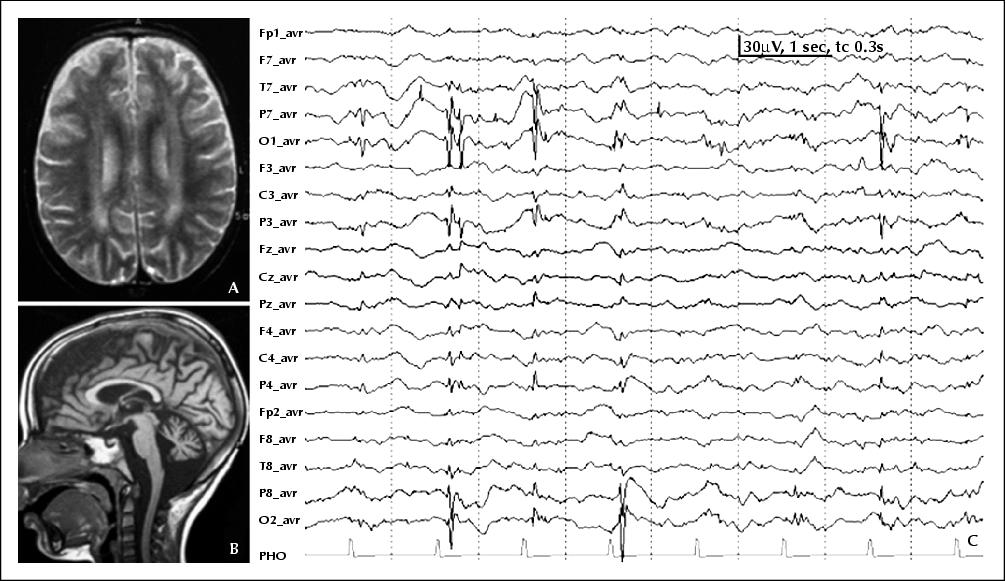
Figure 4 Late infantile neuronal ceroid lipofuscinosis. A) Axial T2w MRI demonstrating periventricular hyperintense white matter changes and cortical atrophy. B) Sagittal T1w MRI showing supra- and infratentorial atrophy. C) EEG (average reference) with slow photic stimulation (1 Hz) and associated spike-wave complexes over the occipital region.
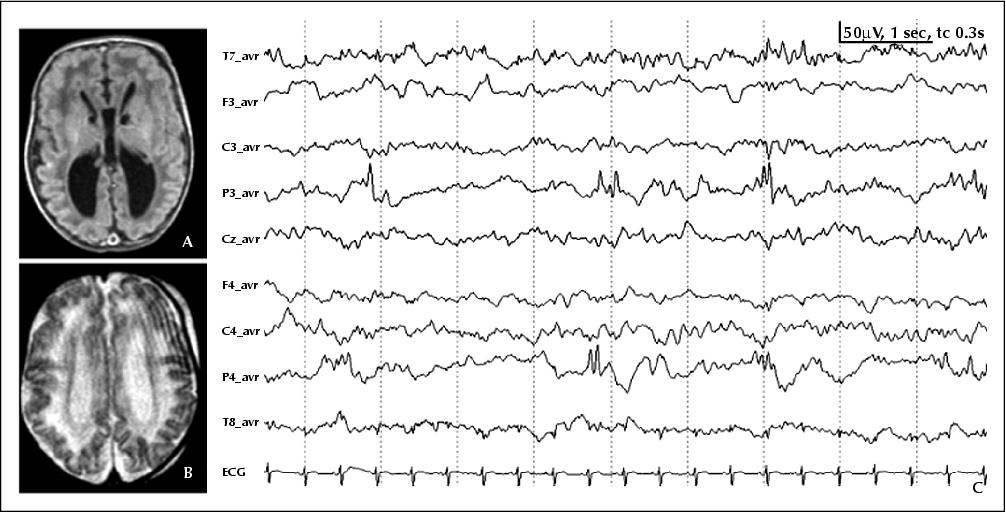
Figure 5 A) T1w and B) T2w MRI of an infant with Zellweger syndrome demonstrating polymicrogyria of the central region and bilateral cysts in the caudothalamic notch. C) EEG (average reference) of the same patient with polyspikes over both parietal regions.
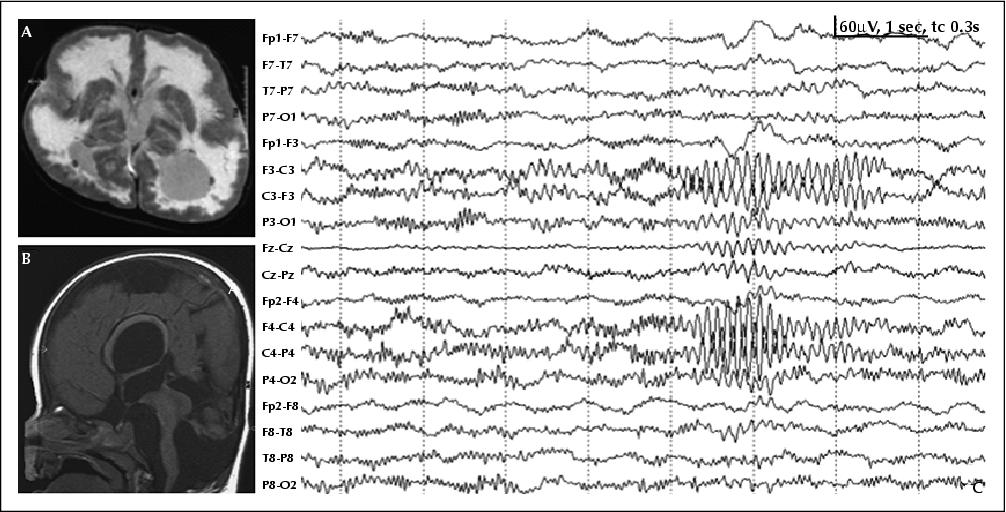
Figure 6 A) Axial T2w MRI of a patient with Walker-Warburg syndrome. Note the diffusely hyperintense abnormal signal of the entire white matter and the cobblestone lissencephaly. B) Sagittal T1w image demonstrating a small, malformed cerebellum and hypoplastic pons and brainstem. C) The EEG (bipolar longitudinal montage) shows abnormal beta activity over the posterior brain regions and a group of 8, Hz alpha activities centroparietally.
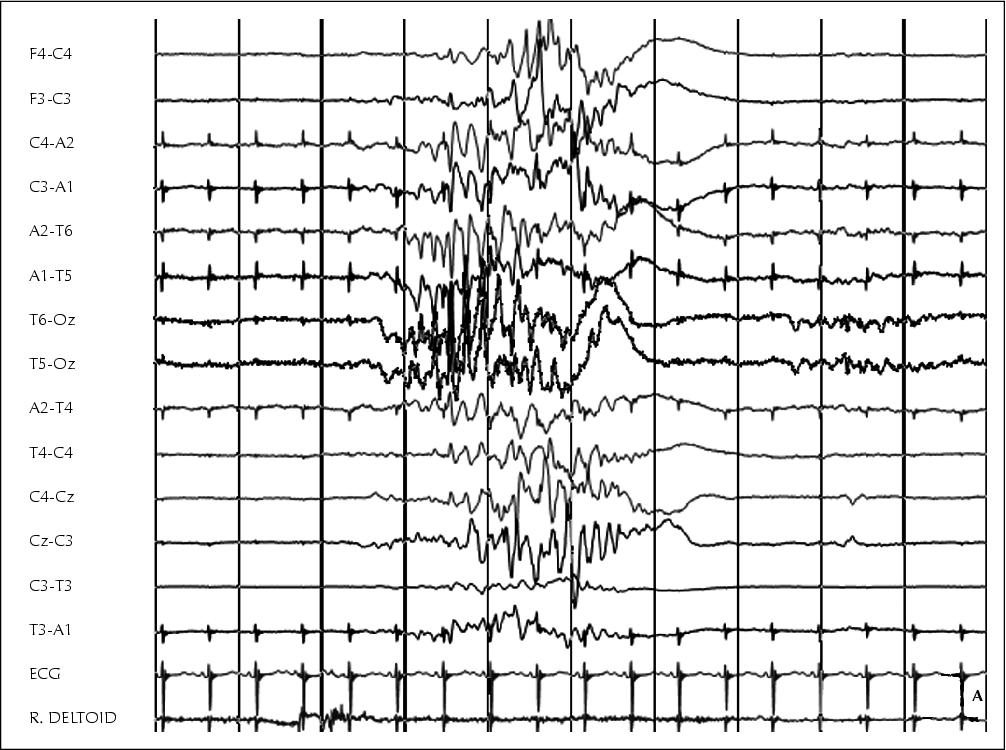
Figure 7 EEG of an infant with pyridoxal phosphate-dependent epilepsy. A) EEG before therapy demonstrates a burst-suppression pattern. B) After initiation of therapy with pyridoxal phosphate, EEG has normalised (in wakeful state; movement artefacts).