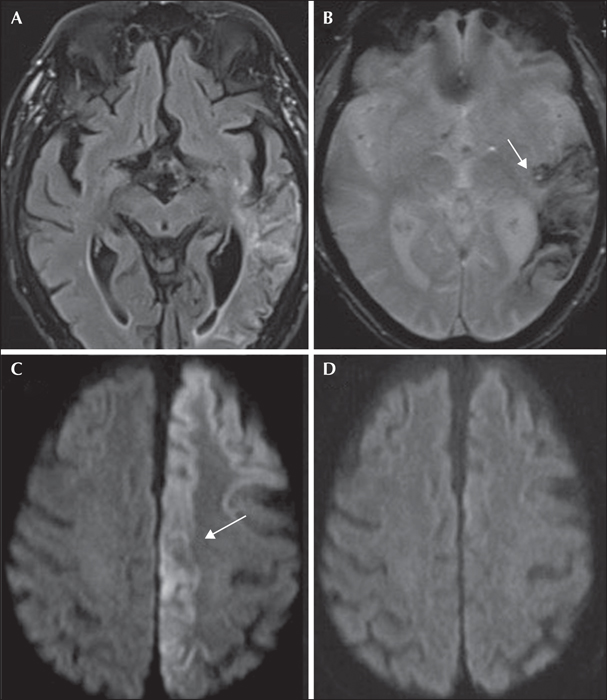
MRI findings in a 73-year-old man with status epilepticus, two years after a left middle cerebral artery ischaemic stroke with haemorrhaging. (A) FLAIR sequence showing a left temporal lobe stroke. (B) Subsequent haemorrhagic transformation of the acute ischaemic lesion (white arrow). (C) Late-onset seizures (status epilepticus), occurring after two years, are associated with DWI restriction in the left cortex in a non-vascular territory involving the frontal and parietal cortex (block white arrow); (D) complete resolution of DWI findings after two weeks.
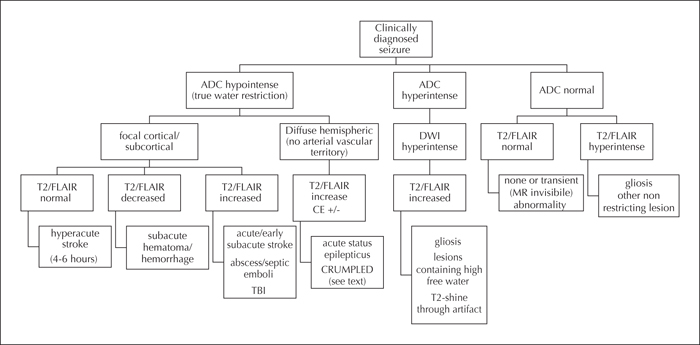
Flowchart for MR signal analysis in patients with an acute seizure. We propose to start with the analysis of apparent diffusion coefficient (ADC) maps. Hypointense lesions on ADC is a reliable sign of true water restriction, which could be due to cytotoxic oedema, hypercellularity or lesions with low water content (e.g. clot, bacterial abscess) lesions. Hyperintensity on both ADC and trace images are characteristic of increased local water content, i.e. vasogenic oedema or gliosis (unless it is a T2 shine-through artefact). These lesions will show increased signal on T2/FLAIR which may or may not be enhanced on gadolinium-enhanced images. This flowchart can be meaningful if carefully analysed in combination with clinical history, patient symptoms and EEG findings. There are no hard and fast rules for differential diagnosis. A close relationship with the neuroradiologist is warranted.
Stroke is one of the commonest causes of seizures and epilepsy, mainly among the elderly and adults. This seminar paper aims to provide an updated overview of post-stroke seizures and post-stroke epilepsy (PSE) and offers clinical guidance to anyone involved in the treatment of patients with seizures and stroke. The distinction between acute symptomatic seizures occurring within seven days from stroke (early seizures) and unprovoked seizures occurring afterwards (late seizures) is crucial regarding their different risks of recurrence. A single late post-stroke seizure carries a risk of recurrence as high as 71.5% (95% confidence interval: 59.7-81.9) at ten years and is diagnostic of PSE. Several clinical and stroke characteristics are associated with increased risk of post-stroke seizures and PSE. So far, there is no evidence supporting the administration of antiepileptic drugs as primary prevention, and evidence regarding their use in PSE is scarce.