Magnesium enhances the beneficial effects of NK1 antagonist administration on blood–brain barrier permeability and motor outcome after traumatic brain injury
Volume 30, numéro 3, July-August-September 2017
Ex vivo imaging of Evans blue (EB) autofluorescence in brains of naive control rats and injured (non-treated) rats at 1 h, 5 h, and 24 h post-TBI. The naive brain shows some low EB autofluorescence in the lateral, third, and fourth ventricles where the choroid plexuses, known to lack BBB, are located. Note the qualitative increase in EB autofluorescence with time in the injured brain.
Evans blue (EB) concentration in brains of naive control animals and injured animals perfused at 1 h, 5 h, and 24 h post-TBI. *** = P < 0.001 versus naive animals; n = 6 per group.
Ex vivo imaging of Evans blue (EB) autofluorescence in brains at 5 h post-TBI of non-treated animals and animals treated with either the NK1 antagonist (n-acetyl tryptophan; NAT), MgSO4 or combined NAT + MgSO4. The images show reduced EB autofluorescence after TBI in all treated animals compared to non-treated animals.
Evans blue (EB) concentration in brains at 5 h post-TBI of non-treated animals and animals treated with either the NK1 antagonist (n-acetyl tryptophan; NAT), MgSO4 or combined NAT + MgSO4. *** = P < 0.001 versus non-treated animals; n = 6 per group.
Ex vivo imaging of Evans blue (EB) autofluorescence in brains at 24 h post-TBI of non-treated animals and animals treated with either the NK1 antagonist (n-acetyl tryptophan; NAT), MgSO4 or combined NAT + MgSO4. Note the marked reduction in EB autofluorescence after TBI in combined NAT + MgSO4 treated animals.
Evans blue (EB) concentration in brains at 24 h post-TBI of non-treated animals and animals treated with either the NK1 antagonist (n-acetyl tryptophan; NAT), MgSO4, or combined NAT + MgSO4. ** = P < 0.01 versus non-treated animals; *** = P < 0.001 versus non-treated animals; † = P < 0.05 versus NAT or MgSO4 treated animals; n = 6 per group.
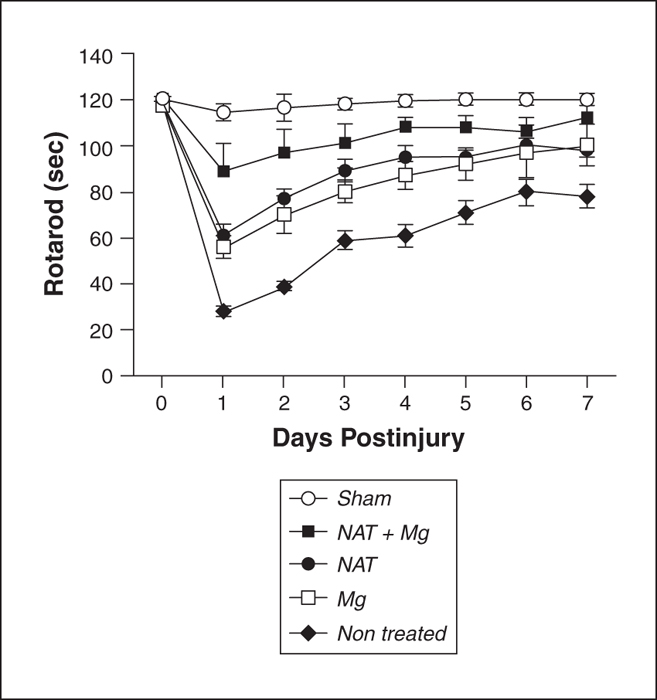
Motor performance (rotarod) scores over 7-day post-TBI in sham, injured (non-treated), and injured animals treated with either the NK1 antagonist (n-acetyl tryptophan; NAT), MgSO4 or combined NAT + MgSO4. All treated groups performed significantly better (P < 0.001) than non-treated animals. Animals treated with combined NAT + MgSO4 performed significantly better (P < 0.05) than animals treated with either compound alone. For clarity, significance symbols have been omitted; n = 6 per group.
The current study investigated whether adding magnesium to an NK1 tachykinin receptor antagonist after traumatic brain injury would enhance efficacy to further reduce blood–brain barrier permeability and improve functional recovery compared to either treatment alone. Sprague-Dawley rats were injured using the impact acceleration model of diffuse brain injury, and received either no treatment, MgSO4 (30 mg/kg IV), the NK1 antagonist n-acetyl L tryptophan (2.5 mg/kg IP), or both agents combined. Animals were then killed at either 1, 5, or 24 h postinjury for determination of blood–brain barrier permeability using previously administered Evans blue dye or assessed for functional outcome over a 1-week period using the rotarod motor test. As expected, both MgSO4 and n-acetyl L tryptophan significantly reduced blood–brain barrier permeability and improved functional outcome. However, combined n-acetyl L tryptophan and MgSO4 was more effective at reducing blood–brain barrier permeability (P < 0.05) and improving functional outcome (P < 0.001) compared to the individual compounds. Our results demonstrate that combination therapy with magnesium and an NK1 antagonist may be a more effective therapy for TBI than either compound administered alone.