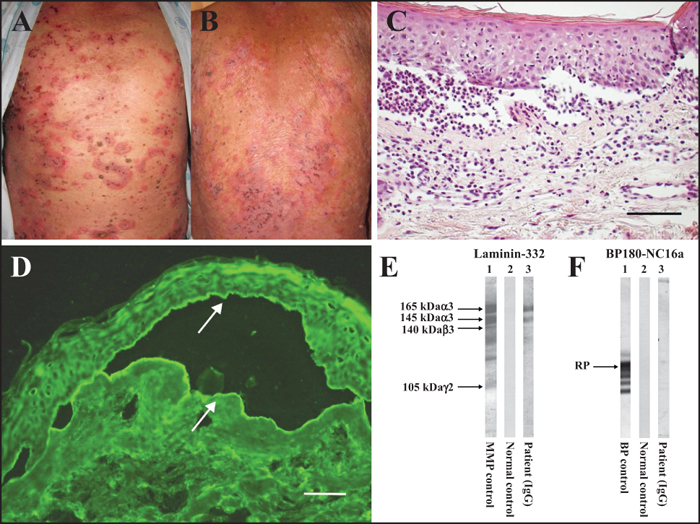
Clinical and histopathological features, indirect immunofluorescence, and immunoblotting studies. A, B) Clinical features. Urticarial plaques and blisters with annular or target-like configuration, often developed on cured psoriatic plaques on the back. Some evolved to erosions and crusts. C) Histopathological examination of an erythematous lesion of the abdomen showed a subepidermal cleft containing mainly neutrophils and lymphocytes, and perivascular infiltration in the dermis (hematoxylin-eosin staining; scale bar: 100 μm). D) Indirect immunofluorescence showed IgG deposits on both the epidermal (upper arrow) and the dermal sides (lower arrow) of 1M-NaCl-split skin (titre: 1:10) (scale bar: 100 μm). E) Immunoblotting on purified human laminin 332 revealed a reaction of control anti-laminin 332-type mucous membrane pemphigoid serum to all the α3 subunits (corresponding to the 165 kDa and 145 kDa protein band doublet), the β3 subunit (140 kDa), and the γ2 subunit (105 kDa) (lane 1), while a normal control serum showed negative results (lane 2). Our patient's serum (lane 3) reacted with the 165 and 145 kDa proteins, corresponding to the α3 subunit of laminin 332. F) In immunoblotting studies for the BP180 NC16a recombinant protein (RP), a positive control BP serum (lane 1), but not normal control serum (lane 2), reacted with the RP. Our patient's serum showed very weak reactivity with the RP (lane 3). BP: bullous pemphigoid.
Autoimmune bullous diseases (AIBDs) are occasionally associated with psoriasis vulgaris; the most prevalent among them is bullous pemphigoid (BP), followed by anti-laminin γ1 (p200) pemphigoid [1]. The association of anti-laminin 332 pemphigoid with psoriasis is very rare, and only one such case has been reported in the literature in a Japanese man [2]. Herein, we report a patient with this association.A 78-year-old Japanese man was referred to our hospital for generalized blistering. He had had [...]